Essential point-of-care tests for veterinarians, part 2: The tFAST3 scan


This is part 2 in a 2-part series. Read part 1 here.
tFAST3 scans or (thoracic) focused assessment for sonography trauma scans, as with the abdominal counterpart, help us identify fluid and other abnormal findings within the thoracic cavity. We can check for fluid and evaluate the heart and lungs for common problems. An invaluable skill, tFAST exams provide a window into the thorax and may help guide additional diagnostics, therapies, and more.
What’s all the fuss about tFAST3 scans?
In the article “Essential point-of-care tests for veterinarians, part 1,” we discussed the origins of the focussed assessment sonography trauma or FAST scan in veterinary medicine. Initially, beginning as an assessment of the abdomen after blunt force trauma, with the main goal of free-fluid identification. The then aFAST scan expanded to assess not just for trauma but for trauma, triage, and tracking.
But free fluid can also occur in the thoracic cavity, so the tFAST3 scan, or thoracic focussed assessment sonography trauma, triage, and tracking emerged.
With practice, in addition to using the aFAST3 exam, evaluation of the thorax allows additional disease identification, including free fluid, heart masses, pericardial effusions, lung pathology, and more.
Benefits of tFAST3 scans
Dr. Lisciandro, one of the pioneers of the aFAST3 and tFAST3 scans and the veterinarian responsible for developing Vet BLUE® and Global FAST®, has two key sacred utterances5(pp1 & 4),10
- Doing only one view (of a radiograph or an ultrasound) equates to no view at all
- tFAST3 simply acts as a continuation of the physical exam in any patient with suspected or known abnormalities
Situations that benefit from a tFAST3 scan
In what situations may we consider using a tFAST scan in a patient?3–5,10 Consider using in
- Any patient with blunt force trauma
- Any patient with penetrating trauma
- Any anemic patient
- Patients with indeterminate hypotension
- Patients at-risk for post-op pneumothorax (PTX)
- Identify and monitor cardio- and non-cariogenic pulmonary edema
- Any patient in respiratory distress
- Any patient with a history of collapse (episodic/current)
- Any patient with known heart disease, acutely decompensating (left atrial tears, for example)
- In the monitoring of any effusion or PTX
- For serial patient monitoring with initial rehydration and subsequent hospitalization. Assess for continued dehydration, deterioration, improvement, or overhydration
- In cases of vomiting – Dr. Lee3 notes that frequently, patients with pericardial effusions have vomiting as the only clinical sign. Sure many have typical collapse or weakness, but if you hear muffled heart sounds (or none) in a vomiting patient, consider a tFAST scan. The only other reason to hear muffled sounds would be significant dehydration.
- Consider using it as a pre-anesthetic screening in at-risk patients
Remember that respiratory distress can occur secondary to non-respiratory tract diseases such as significant fevers, hemoabdomens, anaphylaxis, and more.5(p4) Furthermore, recollect that patients who collapse may present 100% normal but could have had blood pressure, heart rate, and/or mentation changes that go unnoticed by the owner, by you and your staff, or aren’t present at the time of evaluation.
Want more clinical and industry news from IndeVets? Sign up here.
A tFAST scan can…
- Detect a PTX quickly with minimal patient stress
- Assess a PTX’s severity – Severe, moderate, or mild in nature
- Evaluate lung parenchyma for pathology
- Assess heart contractility, thereby assessing volume status
- Evaluate for pericardial and pleural effusions
- Evaluate for life-threatening cardiac tamponade
You found what on your tFAST3 scan?
Patient positioning
Ultimately, the position is whatever is most comfortable and tolerated by the patient. Once skilled with the probe, lateral, sternal recumbency, or standing can glean valuable information and a full tFAST assessment.
However, dorsal recumbency increases the risk of decompensation and should not be used.4,10
The stable respiratory patient
Right lateral recumbency is preferred because most views can easily be seen via this position. While right lateral may be selected, either provide information for four of the five acoustic windows. The final window requires sternal recumbency.
The unstable respiratory patient
For these patients, let them be your guide.
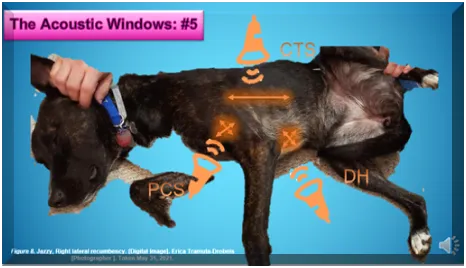
Check out Figure 1 showing Jazzy in right lateral recumbency and the approximate probe transducer locations.
One tip by Dr. Lisciandro when in sternal, to improve the ultrasound probe’s movement may be helpful to you. He recommends using a rolled-up towel placed beneath the patient’s front legs when sternal to elevate the sternum off the examination table.4
More from IndeVets: 10 tips for new vet grads we wish we knew
So, where do we put that probe?1,4,6–9,10(p)
Let’s now discuss the tFAST’s five acoustic windows. Again, I reiterate Dr. Lisciandro’s mantra, “1 view is no view.”5 Thus, evaluate at least two views to ensure you properly identify concerns and don’t miss anything critical. While the patient’s stress and clinical picture may dictate that one view be done initially. Once stable, subsequent views should be obtained. Simply failing to check further because you found one problem may cause you to treat the wrong ailment or lead to the patient’s untimely demise.
Again, refer to Figure 1 to demonstrate the ultrasound probe placement for each acoustic window discussed below.
The first and second of the five views represent the left and right Chest Tube Sites (CTS). Then we have bilateral Pericardial Sites (PCS), concluding with the Diaphragmatico-Hepatic (DH) window.
Yes, this DH view we saw in the first article, Part I: the aFAST3 scan. It is our ‘designated hitter,’ playing a role in both aFAST and tFAST scans. Why is that, you ask? When juxtaposed, the liver and gallbladder create a superb acoustic window, thus, permitting the identification of fluid in all three cavities, abdominal, pericardial, and pleural.
Bilateral CTS:
- Ideal Location to ID a PTX
- Found “directly dorsal to the xiphoid process between the eight and ninth intercostal spaces”4(p144). Depending on the size of the pet or in some with a barrel chest, you may need to shift an intercostal space up or down
- Use the probe along the thoracic wall dorsolaterally with your transducer notch cranially (left of your screen)1(p8)
- Basically, it is performed at the chest’s highest point, aka the least gravity-dependent location – this is where free air will rise, helping to ID a PTX
- What do we find in this view? We can rule out a PTX when identifying ultrasound lung rockets*, or we can identify signs of a normal (dry lung) by seeing a glide sign*. A step sign* would suggest radiographs are warranted to determine if pleural space abnormalities or chest wall trauma occurred.
See the definitions box, Figure 2, for further information on words with an *.

Bilateral PCS:
- Key window to allow visualization of pericardial or pleural effusions
- Left-ventricular short axis view permits contractility evaluation
- On initial assessment and serially over time, permits for fluid volume status evaluation
- Place the probe at junctions of ribs by the 3rd, 4th, and 5th intercostal spaces where one can palpate the heartbeat
- The Right to left ventricular ratio (RV/LV) achieved via a long-axis 4-chamber view
- The probe placement in PCS is often described as initially having the marker directed to the elbow with a rotation towards the spine, obtaining the short then long-axis cardiac views4(pp154-155),10
- Before attempting to evaluate for pathology, allow your patient to take several good breaths, ensuring the viewing window remains visible and enabling the patient to relax
- The PCS permits complete heart chamber visualization, minimizing the chance of incorrectly identifying effusions when in fact, you are just seeing normal anatomy
And the single DH view, our designated-hitter view
- Remember, in the aFAST3 article, we discussed the ability of the liver and gallbladder to provide a great acoustic window for the detection of fluid. Not only does it allow for cranial free-fluid assessment in the abdomen, but this view minimizes air interference, providing a great window into the thoracic cavity. Top that with being well tolerated even in respiratory distress patients, further explaining its designated-hitter status.
- One of the best views, if not the best to check for pericardial and pleural effusions
- Allows assessment of the caudal vena cava and liver vessels for evidence of fluid overload, congestion, or right-sided heart concerns
- Can allow evaluation of the accessory lung lobe, pleural space, and some cardiac structures
- In this position, when evaluating the chest, you need to ensure sufficient transducer penetration depth. Dr. Lisciandro4(p157) recommends ensuring that the thorax occupies 25-33% of the far field.
- Remember that even when completing a tFAST scan, you have a window into the abdomen, so don’t forget to evaluate the structures visible from this view. You don’t want to miss something simply because you didn’t look.
- Recall from the aFAST3 article that the probe for this view is facing the patient’s head just below the xiphoid. Going just subxiphoid may benefit smaller patients or those with respiratory distress.
Determining a wet or a dry lung4(p152),10
Briefly, a dry lung constitutes the normal lung. We declare the lungs normal upon visualization of the A-lines* with a glide sign.* However, when we see B-lines or ultrasound lung rockets,* we identify a patient with wet lungs.
Finding B-lines in the face of trauma leads to a presumptive diagnosis of pulmonary contusions until proven otherwise. Contrast this to the non-trauma patient, where we presume them to be interstitial edema. We cannot differentiate just from their appearance between noncardiogenic or cardiogenic origins.
Who cares, you may ask? However, edema must penetrate the individual alveoli to actually auscult wet lungs. Ideally, we want to know that edema develops before reaching the point where we hear it with a stethoscope. Evidence of B-lines demonstrates true edema earlier than crackles develop.
Everything you want to know about monkeypox for veterinarians
Differentiating pericardial and pleural effusions1,4,5,10
Without tapping the chest and sampling the fluid, you cannot characterize an effusion via ultrasound. A tFAST scan simply helps you discern its presence.
Remember that fluid between the lung and body wall puts pressure on the lung tissue causing it to collapse (atelectasis). We can appreciate atelectasis by imaging “triangular echogenic structures floating within the effusion.”1(p8)
Obviously, finding pulmonary effusion constitutes a significant medical issue. However, it does provide enhanced visibility of the lung and heart. So, when present, you can take advantage of the improved visibility to evaluate the health of the structures.
Going into details about the differences is beyond the scope of this article. However, ultrasound represents the gold standard for detecting pericardial effusions. A pericardial effusion will be seen as fluid contained, while pleural effusion tends to be unrestrained and uncontained.5(p3),10
What about air where it doesn’t belong?
Up to this point, the focus has been on finding fluid in the cavities of concern or fluid within the pulmonary tissue. However, what if we were to expect air where it shouldn’t be? Pneumothoraces occur spontaneously in some breeds and after trauma or secondary to other underlying diseases.
Identifying a PTX on ultrasound may help determine your course of action. You still may want to confirm it on radiographs but may need to stabilize the patient first.
The 1/3s rule for a PTX5,8,10
Using a tFAST exam, we can approximate the degree of air present in a PTX patient. By evaluating the degree of air present in a PTX and gauging the severity, we allow the determination of the need for a thoracocentesis.
Additionally, knowing the degree of air at the start permits monitoring to determine if the patient remains static or becomes worse or if you are reaching clinical improvement.
We quantify the PTX’s severity of a patient in sternal recumbency based on where the air is found:
- Trivial Only the upper (dorsal) 3rd of the chest is involved;
- Moderate, concerning The middle 3rd involved;
- Severe, concerning Lower (ventral) 3rd involved.
A tip from Dr. Lisciandro4(p148) advises upon any positional patient change, allow the pet to take five good breaths before starting to scan again. This permits air redistribution as the patient settles into a new position.
Constraints and hindrances to tFAST evaluations3,4,10
Things to remember when performing tFAST evaluations include:
- As with aFAST scans, make sure you don’t over-interpret findings. Make sure you are truly comfortable identifying the normal vs. the abnormal.
- Make sure you have complete information; one view is never sufficient. You may need to use a combination of different modalities to gain a full clinical picture, but make sure you do more than one view.
- Refer when appropriate; get confirmation of findings by a specialist – a complete thoracic ultrasound and or echocardiogram
- Ensure adequate transducer pressure, so you don’t displace fluid.
- Subcutaneous emphysema, common in the face of trauma, could create problems with ultrasound and wave transmission. However, applying sufficient pressure to the tissue generally allows the air to displace enough to visualize and rarely interferes with the tFAST exam or in identifying abnormalities.4(p153)
- Remember that low blood pressure or dehydration for low-volume effusions may prevent visualization of the fluid. Be careful not to presume no fluid exists just because you didn’t find it. If the clinical picture fits, you may need to do that other view, use another modality, or serially repeat the scan to recheck over time.3
But always remember that any test remains only as good as the person performing it and interpreting the findings.
Treating feline idiopathic cystitis (FIC): A how-to
Practice, practice, practice
Remember, even once adept at the skill of performing a tFAST scan, you want to provide your patient and the owners with your best foot forward.
Always advise clients that a tFAST scan isn’t equivalent to a full ultrasound, that you aren’t measuring organs and evaluating at the level of detail a specialist would with a full ultrasound.
Always offer a referral to a specialist. While this isn’t necessary in many cases, you cover yourself liability-wise and ensure owners fully understand what the FAST scan tells them. Explain why a full thoracic ultrasound or echocardiogram is still warranted despite your already completed work.
The key remains to ensure you practice, learn the normals, know the abnormals, and know what to do with the information and techniques you perform.
Always confirm findings with more than one view and/or different modalities. Remember that just because you complete this scan, it doesn’t take the place of thoracic radiographs or a full thoracic ultrasound. Still, it provides a window into the patient, allows rapid estimations of disease severity, and provides a place to focus your attention and client recommendations.
This article just scratches the surface, describing in very broad terms the benefits of a tFAST scan. You will want to pick up a textbook or take one of the many online classes that further elucidate the various acoustic windows, the finesse needed to acquire diagnostic images, and the knowledge to properly interpret the normal vs. abnormals.
Parting thoughts
Whether you evaluate the abdomen or the thorax, FAST3 scans can provide a wealth of information. Though originally, the FAST scan was all about blunt force trauma and free fluid assessment, you should have a good understanding of how it has evolved into much more than that.
Upon scanning your patient, you may find no abnormalities or more than you bargained for, but you can deliver valuable findings and feedback to your clients. When refined, your ability to evaluate for more than just free fluid, confirm your suspected concerns, and monitor a patient’s progress, are invaluable.
Erica Tramuta-Drobnis, VMD, MPH, CPH is the Founder & CEO ELTD of One Health Consulting, LLC, as well as a freelance writer, consultant, researcher, public health professional and small animal veterinarian.
More from IndeVets:
Our guide to essential veterinarian resources
Your top 5 questions about relief work, answered
References
- Hammel PE, Berry CR. Sonography Assessment: Overview of AFAST and TFAST. Today’s Veterinary Practice. Published November 2, 2018. Accessed July 21, 2022. https://todaysveterinarypractice.com/radiology-imaging/sonography-assessment-overview-of-afast-and-tfast/
- Husain LF, Hagopian L, Wayman D, Baker WE, Carmody KA. Sonographic diagnosis of pneumothorax. J Emerg Trauma Shock. 2012;5(1):76-81. doi:10.4103/0974-2700.93116
- Lee J. Emergency Medicine/Toxicology. In: Emergency Medicine/Toxicology. Delaware Valley Academy of Veterinary Medicine; 2020.
- Lisciandro GR (Ed). Point-of-Care Ultrasound Techniques for the Small Animal Practitioner, 1st Edition. First. John Wiley & Sons, Incorporated; 2014.
- Lisciandro GR. Thoracic FAST (TFAST®) for Trauma, Triage, and Tracking. In: Southwest Veterinary Symposium, 2017. Southwest Veterinary Symposium; 2017:6. https://wendyblount.com/articles/ultrasound/2Article-TFAST-2017SWVS-Lisciandro.pdf
- Lisciandro GR. Case-Based Applications of Thoracic Fast (R)- Trauma, Triage, and Tracking- and the Accurate Diagnosis of Pleural and Pericardial Effusion and its TFAST Echo views. In: Latin American Journal of Veterinary Medicine for Emergency Intensive Care (LAVECC) Conference. LAVECC; 2018. Accessed July 26, 2022. https://fastvet.com/wp-content/uploads/2018/09/03-General-Final-TFAST-for-PE-and-PCE-FASTVet-Cornell-Billings-LAVECCS-2018-TFAST.pdf
- Lisciandro GR. Sonography in the Emergency Room. In: Drobatz KJ, Hopper K, Rozanski EA, Silverstein DC, eds. Textbook of Small Animal Emergency Medicine. First. John Wiley & Sons, Ltd; 2018:1183-1194. doi:10.1002/9781119028994.ch182
- Lisciandro GR, Mazzaferro E. Global FAST®: assessing patient volume status. Vetstream Canis. Published online 2020. https://www.vetlexicon.com/treat/canis/freeform/global-fast%C2%AE-assessing-patient-volume-status
- Lisciandro GR. Proactive Lung Ultrasound: The Vet BLUE & the Tale of Four Felines. In: American Association of Feline Practitioners. American Association of Feline Practitioners; 2018. Accessed July 26, 2022. https://wendyblount.com/articles/ultrasound/2Article-GFAST-2018AAFP-FelineCases-Lisciandro.pdf
- Tramuta-Drobnis EL. The Usefulness of a tFAST3 Exam as a Point-of-Care Test. In: ER Fast Scan Mastery. First. Vet Ultrasound Training. Scan School Vet Ultrasound Training; 2021:Thoracic fast scan what’s the difference? Accessed June 2, 2021. https://vetultrasoundcourse.com/members-area-access1606238229299