Weird Case Files: “A pain in the leg” diagnosis


Meet Josie, a 2-year-old FS Belgian Malinois
This edition of “Weird Case Files” highlights Josie who presented to me for significant lameness on the right hind limb. Josie is an incredibly active, high-energy dog, and her owner does a great job at providing outlets for her energy. She has that classic drive that makes the Malinois a great working dog and means she will chase a ball until she physically can’t get up anymore! What Josie is not great at is resting, and the owner reported worsening bouts of intermittent lameness, as well as an area of swelling on the right hind limb that seemed to come and go since she was about 1 year of age. He had mentioned this at a previous appointment, but Josie’s lameness was not as significant at that time, and a soft tissue injury of some kind was presumed. There was no reason to consider a more sinister diagnosis at her age. Josie’s physical exam was normal at our initial appointment, other than significant clinic anxiety, a toe-touching lameness in the right hind limb, and an obvious asymmetry between her distal tibias.
Her right distal tibia was noticeably thicker than her left, but the “swelling” was certainly not soft tissue. It felt extremely firm and palpated like bone. There was no obvious associated subcutaneous edema, no obvious external wound, and the hock maintained a normal range of motion. Josie was already quite stressed and now clearly in pain as I examined the distal right tibia. I knew I wanted radiographs after my initial examination, so sedation was in order. Oh, the combination of butorphanol and dexmedetomidine, how I love thee for settling our most anxious patients for imaging! Once sedated, we got a rectal temperature, which was initially 105° F, but came down to 103° F by the time we reversed her sedation. I didn’t learn much more from the affected area upon the sedated exam, but what I saw on her initial set of radiographs made my heart sink to the floor.



I saw an aggressive bone lesion, with proliferative cortical/periosteal changes starting in the diaphysis, worsening down the metaphysis, and not affecting the tibiotarsal joint. There was also a general loss of bone density from where the cortical changes started, moving distally. These are the kind of radiographs that break your heart, make you want to throw up, and involuntarily tighten all your sphincter muscles simultaneously. There are only two things we see in medicine that can cause this kind of radiographic bone pattern – cancer and infection – and you cannot tell the difference between the two solely on radiographic appearance. “Okay, well Josie is two years old,” I thought once I regained the ability of rational thought. Her owner had also reported intermittent lameness/swelling for the past year. I’ve seen plenty of osteosarcoma (OSA) cases, but never in a 1-year-old dog, never with this strange intermittent swelling history, and they have never felt this incredibly dense on palpation. I remember after euthanizing one OSA case I was able to bend the affected bone like rubber. Knowing how hard this dog has continued to exercise over the past year, how has she not broken this bone? Well, if she has had clinical OSA for at least a year, she should have pulmonary metastasis, right? Cue, the thoracic radiographs!


Shoot! Why did there have to be something in her lungs?! A 3.3 cm mineralized focal nodule was present in the left lung field, overlying the heart on the lateral image. Not ideal, but the rest of her lung fields were clear. I’ve also seen pulmonary metastasis from OSA before, and it typically presents with the classic “snow globe appearance,” a diffuse nodular pattern representing areas of macroscopic disease after microscopic spread through the bloodstream. This was not that.
At this point, I had to update the owner. I don’t know what kind of previous radiology experience this man had, but the look on his face after seeing the radiographs let me know he understood exactly what this looked like before I even started talking, and before I finished there were tears in his eyes. He shared with me that this dog was his entire world. It’s just him and her all day every day, and the thought of losing her so young was devastating. Now I’ve got tears in my eyes. Please don’t let this be cancer! I reminded him that at this point we don’t have a diagnosis, but this bone looks scary and is at risk for pathologic fracture. We are currently straddling the differential fence between neoplasia and infectious osteomyelitis, but she has age on her side. Finding a mass in the chest after seeing a bone like this is troubling for cancer, but there are details here that don’t add up for metastasis. I recommended sending the images out for radiologist review, submitting screening blood work, and getting a biopsy of the lesion. The biopsy would be done under general anesthesia after seeing her blood work results, and hopefully we would have her radiology report back at that time. I was hoping maybe I would find supportive evidence of infection in her cell counts. Maybe her temperature was more than just severe clinic anxiety! Maybe the radiologist would see past the glaring radiographic red flags for neoplasia and tell me to hunt for underlying infection.
Infectious osteomyelitis comes in three different varieties – bacterial (Brucella canis, Bartonella, Clostridium spp, Staphylococcus spp, Pseudomonas spp, Pasteurella spp, etc.), fungal (Aspergillus, Blastomycosis, Coccidioides, Histoplasmosis, Cryptococcus), and parasitic (Hepatozoonosis, Leishmaniasis). I figured I could at least start to cover her for possible bacterial osteomyelitis while we waited on diagnostic results. I sent her home that day on a course of Clavamox. I sent home Carprofen and Gabapentin for pain relief.
Results:
- CBC – unremarkable
- Chemistry – Unremarkable, other than a mild creatinine elevation of 1.7 mg/dL in the face of a normal SDMA
- Heartworm Ag negative
- Radiology report – Annoyingly very doom and gloom…They didn’t even mention the possibility of infection!
Conclusion: Aggressive bone lesion of the distal right tibia. Neoplasia such as osteosarcoma is prioritized. Bone biopsy would be needed to confirm. Pulmonary nodule/mass, likely metastatic neoplasia.
Biopsy:
Though diagnostics up to this point were not getting us any further away from a diagnosis of OSA, a biopsy would at least be definitive for officially ruling OSA in or out. The practice owner veterinarian was the one who performed her biopsy under general anesthesia. He took a sample from the medial aspect of the distal tibia at the widest point of proliferation. He ended up having to use a chisel and mallet to get a good bone sample due to how firm the bone was. For me, this was another check for the “not OSA” column, as I have biopsied OSAs before and have been able to easily get samples with a wedge or punch biopsy as the bone becomes very fragile when lytic.
At this point I also got a little more frustrated at the radiologist report (and myself), as the practice owner veterinarian picked up on a radiographic detail both the radiologist and I missed. There was another affected bone!

One of her caudal vertebrae that could be visualized on her initial set of radiographs showed the same kind of cortical/periosteal proliferative changes and loss of general bone density. I wish I had imaged her entire skeleton after finding this as there may have been more bones affected! Once again, this did not add up for an OSA diagnosis, and after over a month of waiting for decalcification and multiple pathologist reviews later we officially ruled out OSA.
Histopathology report
Microscopic findings:
Right distal tibia: Reactive bone with mild intratrabecular hypercellularity, most suggestive of chronic inflammation/osteomyelitis, possibly mildly pyogranulomatous, with surrounding mild chronic soft tissue inflammation and fibrosis.
Addendum: Five serial deeper step levels of the biopsy specimens were examined. In the deeper sections there were areas of mild intratrabecular increased cellularity. These areas consisted of an admixture of cell types including discernible lymphocytes, plasma cells, macrophage type cells and a few neutrophils. There are also reactive changes in the bone. No infectious agents were seen with routine H&E stain, however an infectious osteomyelitis is possible, and fungal diagnostics should be considered. For thoroughness special stains for fungus and acid fast stains will be examined and results will follow.
Addendum: A PAS and a GMS fungal stain are examined. No definitive fungal organisms are observed. Low numbers of organisms, lack of capturing organisms in the sections or degenerative organisms may not always be identified with special stains and negative results do not rule out fungal infection.
Diagnosis:
We had ruled out cancer with a biopsy report supportive for infectious osteomyelitis, wahoo! Josie, however, was not jumping for joy. Dad was still doing his best to try and rest this high energy dog, but she had shown no clinical improvement after the course of Clavamox. A course of Cefpodoxime was added after her bone biopsy, again with no clinical improvement. Josie remained as painful as ever on the leg, and we continued to manage her pain on Carprofen and Gabapentin. At one point I even added in Amantadine for extra pain relief when the owner was going to be gone on a long road trip with her and she was struggling.
After the histopathology report was finalized, we moved forward with fungal serology, and that’s when it finally happened. The missing piece of the puzzle!
Fungal Serology:
- Histoplasmosis – Negative
- Blastomycosis – POSITIVE!
- Aspergillosis – Negative
- Coccidioidomycosis – Cocci Antibody (IgM) – Negative, IgG screen – Negative, Coccidioides IgG titer – Titer not indicated
Josie was started on Fluconazole 200 mg SID for blastomycosis almost two months after our appointment when her original radiographs were taken. It took over a month to get her off pain medications and see the kind of clinical improvement we were waiting for. We repeated radiographs about 3 months after the first set, which showed a significant, albeit slow, improvement in the right tibia.


The mass in the chest showed almost no change.
The plan for now is for Josie to stay on the Fluconazole for another 3 months and reassess radiographs at that point, with the goal of weaning her off antifungals once the tibia is radiographically normal. The mass in the chest is most likely a fungal granuloma that may or may not change over time due to the degree of calcification present.
What Josie taught me:
Remember all possible differentials at play and don’t jump to conclusions based on previous clinical experiences. You cannot tell the difference between fungal infection and cancer on radiographs! Josie could have been humanely euthanized after those initial radiographs if the wrong pair of highly trained eyes misread them as metastatic OSA and didn’t push for biopsy. Josie could have been euthanized if those same pair of highly trained eyes had taken the original radiology report’s suspected diagnosis and had not performed confirmatory testing. It’s very easy to get neoplastic tunnel vision on a set of radiographs like Josie’s and forget all of the other pieces of the puzzle – the firmness of the bone, the on and off swelling reported by the owner, the other radiographically affected bone, her possible fever, the fact that she only had one solitary lung nodule that appeared calcified instead of a diffuse nodular pattern (which can also be seen with systemic fungal infections). I have seen two other cases of blastomycosis in my career thus far, both when I was a vet student. Each dog was obviously systemically ill, one with severe respiratory disease and one presenting to ophthalmology for horrendous uveitis. Both dogs presented febrile with cell count changes supportive of systemic infection. Josie’s case, on the other hand, never fit these patterns. If it hadn’t been for the worsening asymmetry in her bones she likely would have continued to be treated for presumptive soft tissue injuries. After all, no one would expect to find a bone like this in a two-year-old dog!
I will never forget this case. Josie is the perfect reminder to take a breath and think before jumping to a diagnosis based on your initial interpretation of a set of scary radiographs. It was a long journey to get to her diagnosis and will be an even longer one until that right tibia starts to resemble the left again. It is, however, starting to look like Josie and her Dad may get their happily ever after. Josie’s getting back to her normal Malinois intensity, and Dad gets to enjoy more quality time with his favorite girl.
Blastomycosis – An Overview:
Blastomycosis is infection with Blastomyces spp., which are dimorphic, saprophytic fungi found in soil and organic matter. The states with highest incidence of blastomycosis are Wisconsin, Minnesota, Missouri, Illinois, Michigan, Kentucky, West Virginia, Arkansas, Tennessee, North Carolina, South Carolina, Louisiana, and Mississippi. Other endemic states include Indiana, Iowa, Ohio, Virginia, Georgia, Alabama and Vermont. Josie and I live in Georgia. The annual incidence of blastomycosis is about 1420 cases per 100,000 dogs in a highly enzootic area. Proximity to waterways and exposure to excavation are significant risk factors. Cases occur most often in the fall but may occur any time of the year. Blastomycosis affects many animal species. Dogs and humans are infected most often, but rare infections have been reported in domestic cats, wolves, deer, ferrets, foxes, horses, African lions, dolphins, sea lions, and other species. While localized infections can occur, blastomycosis primarily affects the respiratory system and causes systemic pyogranulomatous disease. Significant mortality and morbidity can occur.
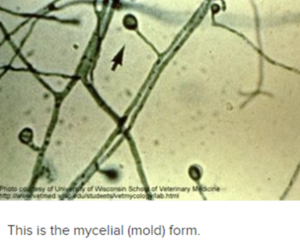
Infection occurs when conidia are inhaled. Incubation at body temperature results in conversion of the conidium/spore of the mycelial form to the yeast stage, which is followed by rapid reproduction via asexual budding.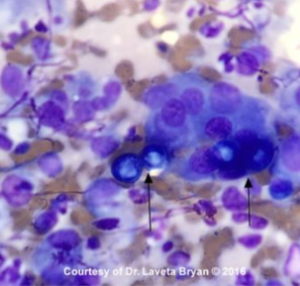

Yeast resist destruction by neutrophils and trigger a pyogranulomatous response. Dissemination can occur via blood and/or lymphatic routes, and can result in granuloma formation in multiple organs, including the upper and lower respiratory tract, reproductive system, central nervous system (CNS), eyes, oral cavity, lymph nodes, joints, bones, and skin.
Pulmonary disease is by far the most common manifestation, but ocular involvement (posterior uveitis, retinal detachment, secondary glaucoma, endophthalmitis, panophthalmitis) is common in dogs and is typically associated with systemic disease. Poor body condition, lymphadenopathy, ulcerated or draining skin lesions, cutaneous/subcutaneous masses, lameness, bone or joint pain, CNS signs, dysuria, hematuria, and/or testicular swelling may also occur.
Typical blood work findings:
- Changes are commonly nonspecific (anemia, leukocytosis, neutrophilia with or without left shift), and reflect the inflammatory response.
- Hypercalcemia secondary to granulomatous inflammation can occur in dogs, and rarely in cats and nondomestic felids. Hyperglobulinemia and hypoalbuminemia are common.
Typical radiographic findings:
- Thoracic radiographs are abnormal in most cases, even in animals without respiratory signs. Diffuse/generalized, unstructured interstitial, “snow storm” pattern is the classic finding (70%) for canine blastomycosis. However, structured/nodular patterns, with or without mixed bronchial and/or focal alveolar disease, may be present. Focal lung masses may occur. Multifocal, nodular disease and solitary, pulmonary or mediastinal masses can be mistaken for neoplasia. Tracheobronchial lymphadenopathy occurs in about 25-30% of cases. Pleural effusion and pneumothorax are uncommon.
- Osteomyelitis from blastomycosis is usually a solitary osteolytic lesion accompanied by periosteal proliferation and soft tissue swelling. Pathologic fractures may be present. Lesions are typically located at ends of long bones, below the elbow and stifle.
Blastomycosis-specific diagnostics available:
- Urine Blastomyces quantitative cell wall galactomannan antigen (EIA) test available from MiraVista Laboratory has a reported sensitivity of 100% and is highly specific. However, cross-reactions can occur with other systemic fungi. The test is not intended to be used as the sole means of diagnosis, and is typically combined with cytologic, radiographic, and other tests. The test can also be performed on serum, plasma, bronchoalveolar lavage, cerebrospinal, and other body fluids. In dogs the EIA test is more sensitive than antibody detection tests by agar gel immunodiffusion (AGID). Urine antigen testing may be negative in dogs with blastomycosis localized to the CNS. A low Blastomyces urine antigen level at time of diagnosis is associated with improved survival times.
- Serum agar gel immunodiffusion (AGID) assays are available through a number of laboratories, screening for antibodies. This test has variable and usually low sensitivity for blastomycosis. Negative AGID results do not rule out disease, especially early in infection. False-negative results can also occur in immunosuppressed patients and those with confined, localized infections. Positive AGID tests are not always indicative of active disease because previous exposure can produce positive results. Diagnosis based solely on positive antibody serology is not recommended.
Prognosis:
Prognosis is good for many canine cases of blastomycosis. Reported recovery rates range from 50-75%, with use of either Itraconazole or Fluconazole. A response rate of 77% was reported in dogs treated with Amphotericin B. However, mortality rates can be as high as 50%, with hypoxemia and respiratory failure being the most common causes of death. Treatment is typically discontinued with resolution of clinical signs, but this can take upwards of several months in severe cases. After discontinuing therapy, animals may be rechecked at 1, 3, and 6 months for evidence of relapse. Relapse rates following Itraconazole and Fluconazole therapy range from 18-24%. Relapses are treated like a new infection.
*Photos and info taken from associate VIN article on blastomycosis.